
Do you have patients that complain of tooth sensitivity but the PA or PAN doesn’t show any pathosis, leaving you and your patient frustrated and not sure how to solve the issue?
CBCT can give you those answers!
Some things to consider:
Periapical Lesion –inflammatory changes of mucosal lining (average mucosal thickening 7.4mm)
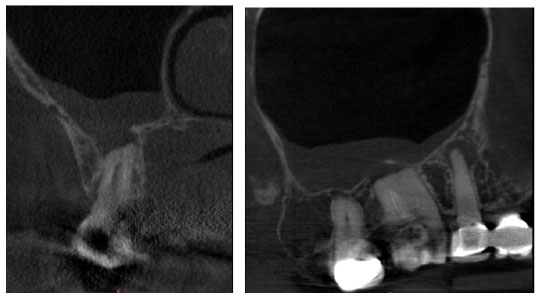
Sinusitis
- Non-Odontogenic in origin but can be odontogenic in origin (more than 50% of the time)
- mostly 1st and 2nd molars
- Palatal root of 1st molar
- Mesiobuccal root of 2nd molar
Sinusitis can happen with or without perforation of the sinus floor.
Infection and inflammatory mediators are able to spread directly via bone marrow, blood vessels and lymphatics to the maxillary sinus.
When the ostium is blocked patient may feel pain the face, eye, nose, and oral cavity, including swelling.
They may experience a vague headache and in Chronic Sinusitis they may complain of postnasal drip, dental pain, and sore throat. Chronic sinusitis can lead to surgical and non -surgical dental and medical treatment.
CBCT is standard of care in medicine for viewing the maxillary sinuses.
Pneumatized Sinus in which the Schneidarian membrane can be easily penetrated by pathegens, and muscles can direct infection into the sinus via soft tissue spaces.
70% of patients diagnosed with maxillary dental infections showed changes in the sinus due possibly to:
- Periapical infection or inflammation
- Periodontal disease
- Perforation of sinus during extraction
- Root tips or other foreign objects forced into the sinus
Four Categories
| NORMAL SINUS |
SINUSITIS OF ODOTOGENIC ORIGIN |
SINUSITIS OF NON-ODONTOGENIC ORIGIN |
SINUSITIS OF UNDETERMINED ORIGIN |
| No mucosal thickening or uniform mucosal thickening <2mm | Soft tissue density mass/ mucosal thickening limited to the area of the tooth or extraction site in question | No evidence of periapical lesions. Mucosal thickening is not limited to any tooth | Periapical lesions or disrupted socket suspect carious teeth. Mucosal thickening is not related to any particular tooth. |
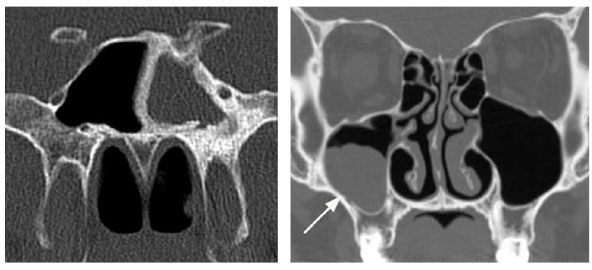
Dome shaped radiopacities are polyps or retention pseudocysts (pathologic entities of non-odontogenic origin.
Could also be:
- Sinonasal polyposis
- Solitary polyps
- Cancer
- Mucocoeles
- Retention cysts
- Antroliths
- Fungal sinusitis
- Sinusitis lacking dental etiology
Could be an endodontically treated tooth or extruded overfilled endo.
Mucosal thickening of 4mm or more was significantly associated with clinical symptoms